



This text is an update to “Psychiatrists’ Response to Human Trafficking.”
Human trafficking is defined as using force, fraud, or coercion to compel an individual into business sex acts or labor against their will.1 Minors involved in business sex are at all times considered trafficked under US federal law. The Motion-Means-Purpose (AMP) Model illustrates the definition of human trafficking (Table 1).2 In 2020, the National Human Trafficking Hotline received greater than 10,000 reports of trafficking within the US.3 From 2016 to 2021, the variety of trafficked individuals worldwide rose by 12%, now numbering over 27.6 million individuals.4
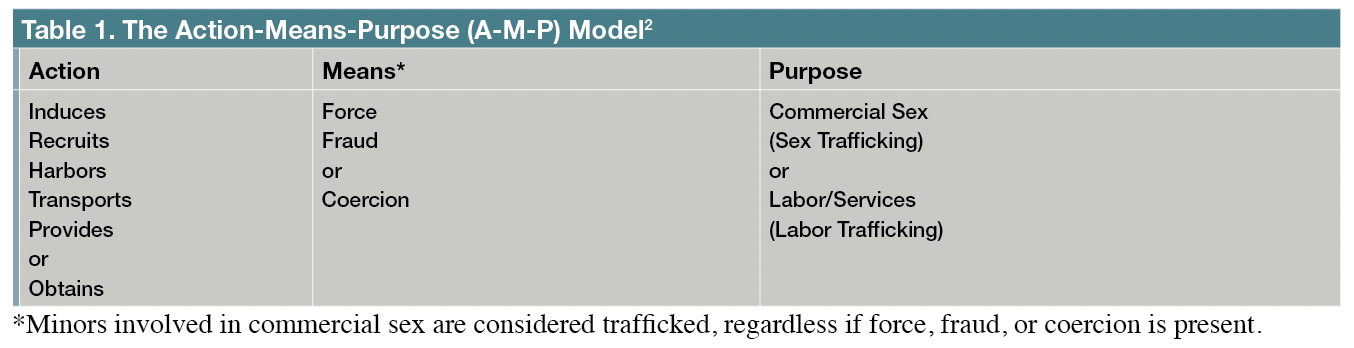
Table 1. The Motion-Means-Purpose (A-M-P) Model2
Traffickers utilize manipulation, grooming, deportation threats, debt, and emotional, financial, physical, and sexual abuse to manage their victims, who often face threats against themselves or their families.5 Most people don’t discover or recognize their situation as trafficking until they exit. It’s due to this fact difficult for trafficked individuals to “just leave” their situation.
Most up-to-date data on human trafficking trends within the US, especially for the reason that COVID-19 pandemic, reveal a major increase in online recruitment and the proportion of people recruited by relations and intimate partners.3 While anyone could be trafficked, certain individuals have heightened vulnerabilities to grow to be trafficked, including those with disabilities, mental illness, substance use issues, unstable housing, financial instability, criminal record or history, and marginalized groups resembling recent migrants, runaway youth, 2S-LGBTQIA+, and ethnic/racial minority communities.3
Trafficked individuals endure psychological and medical consequences which can be complex and long-lasting. Health care systems, including inpatient psychiatric units, could be vital for appropriate identification, intervention, and referral.6 Amongst those with lived trafficking experience, men, those with substance use disorders, and people discharged to temporary housing arrangements usually tend to have readmissions to inpatient psychiatry units.7 One study found that amongst individuals with substance use disorders, alcohol and cannabis were ceaselessly utilized, in addition to polysubstance use, and beneficial broad screening for substance use and a low threshold for referral to specialty services for trafficked individuals.8
Trauma-informed care involves appreciating the impact of the trauma sustained by the patient and understanding that it influences how individuals with trafficking experience engage with service providers and authority figures.9 While on the lookout for general indicators (ie, red flags) and utilizing objective assessment tools might help discover human trafficking, approaching the patient in a trauma-informed manner and listening to their story, provides a greater understanding of their trafficking history. Providing unbiased training on human trafficking to mental health professionals, with accurate portrayals of trafficked individuals, can even improve prompt identification.6
A multidisciplinary approach, including psychiatric care, is pivotal in constantly assessing and treating trafficked individuals’ health and psychosocial needs. Validated assessment tools for health care settings exist for suspected minor victims of sex trafficking but not adults. The Rapid Appraisal for Trafficking (RAFT) tool, a 4-item questionnaire, has shown good sensitivity compared with long, existing, resource‐intensive assessment tools within the emergency department; nonetheless, additional multicenter studies are required (Table 2).10
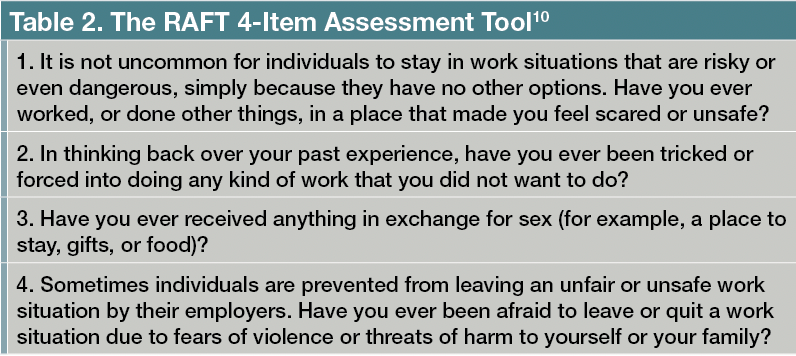
Table 2. The RAFT 4-Item Assessment Tool10
The National Human Trafficking Hotline (NHTH) is obtainable to physicians, health care providers, and patients to report confirmed or suspected trafficking, obtain guidance on the subsequent steps of care, and access social and legal resources. It is obtainable 24 hours, seven days every week, and could be reached by dialing 1-888-373-7888 or texting “HELP” or “INFO” to SMS 233733. Moreover, the National Human Trafficking Training and Technical Assistance Center (a part of the Department of Health and Human Services)11 provides training for health care providers through its SOAR online portal and access to publications, resembling the 2021 Report: Core Competencies for Human Trafficking Response in Health Care and Behavioral Health Systems.12
Case Example
“Mr Lopez” is a 44-year-old man with a history of hypertension and diabetes mellitus type 2 who presented to the medical emergency room with headache, dizziness, nausea, dehydration, and weakness. Because of metabolic abnormalities secondary to dehydration and warmth exhaustion, he was admitted to the inpatient medical floor.
On the second day of hospitalization, psychiatry was consulted after the first team noticed Mr Lopez was dysphoric and tearful. On psychiatric evaluation, Mr Lopez was evasive, guarded, and unwilling to share personal information. Every day follow-up helped Mr Lopez to grow to be more open and trusting towards the team. He reported anxiety, insomnia, anhedonia, decreased concentration, helplessness, hypervigilance, and nightmares that began around 6 months ago after he migrated to the US.
Because of his status as an “undocumented” migrant, job opportunities were limited, and he found an employer who offered him payment, food, and housing on a fruit farm. The farm was secluded, and housing was unsanitary and filled with multiple staff. He described his work duties as highly demanding and noted that he had not been paid despite months of labor. When he raised this issue with the employer, Mr Lopez was threatened with deportation, physical violence, and longer work hours.
The psychiatry team educated Mr Lopez on human trafficking and referred him to a social employee and case manager for housing referral and a psychologist for psychotherapy. He followed up with outpatient psychiatry monthly to treat symptoms of posttraumatic stress disorder. Consequently of his hospitalization, he benefited from mental health and medical services inside a secure and multidisciplinary environment.
Future Directions
Health care professionals across different specialties, especially psychiatrists, need education and training on human trafficking, including the necessity for person-centered, culturally humble, trauma-informed care.13 Mental health clinicians are urged to utilize trauma-informed care to hearken to their patients, construct trust, address safety concerns, empower decision-making and agency, and eliminate biases when working with patients suspected of being trafficked. Developing partnerships between health care disciplines, community partners, and survivor advocates are essential to creating and maintaining a human trafficking response protocol while increasing outreach efforts.
Dr Alhajji is an assistant professor within the Department of Psychiatry and Behavioral Sciences on the University of Miami Miller School of Medicine. Dr Munoz is a PGY-4 Psychiatry Resident on the University of Miami Miller School of Medicine/Jackson Memorial Health System. Dr Padilla is a Consultation-Liaison Psychiatry Fellowship Program Director, and an assistant professor within the Department of Psychiatry and Behavioral Sciences on the University of Miami Miller School of Medicine. Dr Rovner is an assistant professor within the Department of Psychiatry and Behavioral Sciences on the University of Miami Miller School of Medicine.
References
1. What’s human trafficking? Homeland Security. Accessed January 11, 2023. https://www.dhs.gov/blue-campaign/what-human-trafficking
2. The Motion Means Purpose “A-M-P” Model: Polaris Project. National Human Trafficking Hotline. 2012. Accessed January 11, 2023. https://humantraffickinghotline.org/sites/default/files/AMP%20Model.pdf
3. Evaluation of 2020 National Human Trafficking Hotline Data. Polaris. Accessed January 11, 2023. https://polarisproject.org/2020-us-national-human-trafficking-hotline-statistics/
4. International Labour Organization; Walk Free; International Organization for Migration. Global estimates of contemporary slavery: forced labour and compelled marriage. September 2022. Accessed January 11, 2023. https://www.ilo.org/wcmsp5/groups/public/@ed_norm/@ipec/documents/publication/wcms_854733.pdf
5. 2021 Trafficking in Individuals Report. US Department of State. September 14, 2021. Accessed January 11, 2023. https://www.state.gov/reports/2021-trafficking-in-persons-report/
6. Babu J, Boland GM, Salami T. Accurate identification and prosocial behaviors towards human trafficking victims amongst psychology students. Journal of Human Trafficking. 2022;1-15.
7. White CN, Robichaux K. Aspects related to psychiatric hospital readmission for survivors of human trafficking. Journal of Human Trafficking. 2022;1-12.
8. Koegler E, Wood CA, Johnson SD, Bahlinger L. Service providers’ perspectives on substance use and treatment needs amongst human trafficking survivors. J Subst Abuse Treat. 2022;143:108897.
9. Lanehurst A, Gordon M, Coverdale J, et al. Integrating trauma-informed care into clinical practice with trafficked individuals. Bull Menninger Clin. 2022;86(Complement A):44-55.
10. Chisolm‐Straker M, Singer E, Strong D, et al. Validation of a screening tool for labor and sex trafficking amongst emergency department patients. J Am Coll Emerg Physicians Open. 2021;2(5):e12558.
11. SOAR Online. National Human Trafficking Training and Technical Assistance Center. Accessed January 11, 2023. https://nhttac.acf.hhs.gov/soar/soar-for-individuals/soar-online
12. Report: Core Competencies for Human Trafficking Response in Health Care and Behavioral Health Systems. National Human Trafficking Training and Technical Assistance Center. Accessed January 11, 2023. https://nhttac.acf.hhs.gov/resource/report-core-competencies-human-trafficking-response-health-care-and-behavioral-health
13. Alhajji L, Hadjikyriakou M, Padilla V. Psychiatrists’ response to human trafficking. Psychiatric Times. 2021;38(12):67-70.

